
B Vitamins, Brain Health, Cell Protection, Energy, Enzymes, Gut health, Microbiome, Mighty Multi-Vite!, Nucleic Acids, Nutrition, Nutritional Supplements, Supporting Protocols, Video, Vitamin B12
VITAMIN B-12: THE NEGLECTED NUTRIENT

Dec
 I previously wrote METHYLATION CYCLE, GENETICS, B VITAMINS in which I considered in-depth how the Methylation Cycle functions, how genetics affect metabolic pathways, and how B vitamins (including vitamin B-12, folate, vitamin B6, and vitamin B2) are used in Methylation Cycle pathways. In today’s article, I take an in-depth view of what you need to know about Vitamin B-12, including the effects of not having sufficient amounts of Vitamin B-12 in the body.
I previously wrote METHYLATION CYCLE, GENETICS, B VITAMINS in which I considered in-depth how the Methylation Cycle functions, how genetics affect metabolic pathways, and how B vitamins (including vitamin B-12, folate, vitamin B6, and vitamin B2) are used in Methylation Cycle pathways. In today’s article, I take an in-depth view of what you need to know about Vitamin B-12, including the effects of not having sufficient amounts of Vitamin B-12 in the body.
Vitamin B-12 is one of eight B vitamins. It is the largest and most structurally complicated vitamin. It consists of a class of chemically related compounds (vitamers), all of which show physiological activity. It contains the biochemically rare element cobalt positioned in the center of a chemical ring structure.
Vitamin B-12 (also called cobalamin) is a water-soluble vitamin that is involved in the metabolism of every cell of the human body. It is a cofactor in DNA synthesis, and in both fatty acid and amino acid metabolism. It is particularly important in the normal functioning of the nervous system via its role in the synthesis of myelin and in the maturation of developing red blood cells in the bone marrow.

YOUR NEED FOR VITAMIN B12
Vitamin B12 deficiency is thought to be one of the leading nutritional deficiencies in the world. An extensive 2004 study showed that deficiency is a major health concern in many parts of the world, including the North America, Central and South America, India, and certain areas in Africa. It is estimated that 40 percent of people may have low levels of vitamin B-12.
Vitamin B-12 affects your mood, energy level, memory, nervous system, heart, skin, hair, digestion and more. It is a key nutrient regarding adrenal fatigue and multiple metabolic functions including enzyme production, DNA synthesis, and hormonal balance.
Because of vitamin B-12’s extensive roles within the body, a vitamin deficiency can show up in many different symptoms, such as chronic fatigue, mood disorders such as depression, chronic stress, and low energy.
SOURCES OF VITAMIN B12
The only organisms to produce vitamin B-12 are certain bacteria and archaea. Some of these bacteria are found in the soil around the grasses that ruminants eat. They are taken into the animal, proliferate, form part of their gut flora, and continue to produce vitamin B-12.
Products of animal origin such as beef (especially liver), chicken, pork, eggs, dairy, clams, and fish constitute the primary food source of vitamin B-12. Older individuals and vegans are advised to use vitamin B-12 fortified foods and supplements to meet their needs.

Commercially, Vitamin B-12 is prepared by bacterial fermentation. Fermentation by a variety of microorganisms yields a mixture of methylcobalamin, hydroxocobalamin, and adenosylcobalamin. Since multiple species of propionibacterium produce no exotoxins or endotoxins and have been granted GRAS status (generally regarded as safe) by the United States Food and Drug Administration, they are the preferred bacterial fermentation organisms for vitamin B-12 production.
Methylcobalamin and 5-deoxyadenosylcobalamin are the forms of vitamin B-12 used in the human body (called coenzyme forms). The form of cobalamin used in many some nutritional supplements and fortified foods, cyanocobalamin, is readily converted to 5-deoxyadenosylcobalamin and methylcobalamin in the body.
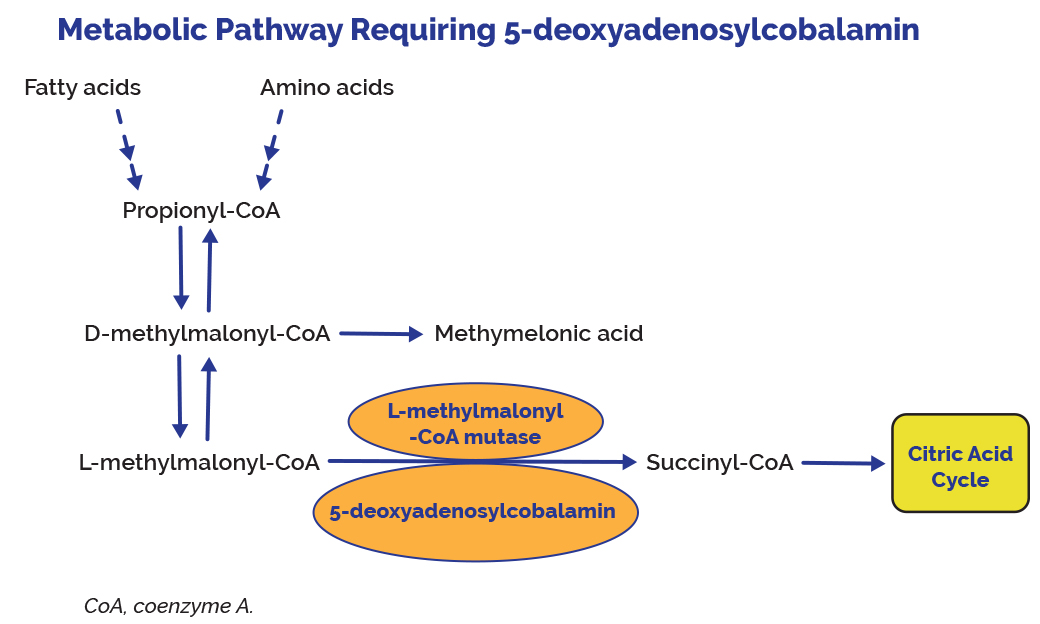
Hydroxocobalamin is the direct precursor of methylcobalamin and 5-deoxyadenosylcobalamin. In mammals, cobalamin is a cofactor for only two enzymes, methionine synthase (MS) and L-methylmalonyl-coenzyme A mutase (MUT).
Unlike most other vitamins, B-12 is stored in substantial amounts, mainly in the liver, until it is needed by the body. If a person stops consuming the vitamin, the body’s stores of this vitamin usually take about 3 to 5 years to exhaust. Vitamin B-12 is primarily stored in the liver as 5-deoxyadenosylcobalamin, but is easily converted to methylcobalamin.
ABSORPTION OF VITAMIN B12
When vitamin B-12 is added to fortified foods and dietary supplements, it is already in free form and, thus, does not require the separation from food protein step. Free vitamin B-12 then combines with intrinsic factor, a glycoprotein secreted by the stomach’s parietal cells, and the resulting complex undergoes absorption within the distal ileum by receptor-mediated endocytosis.
Approximately 56% of a 1 mcg oral dose of vitamin B12 is absorbed, but absorption decreases drastically when the capacity of intrinsic factor is exceeded (at 1–2 mcg of vitamin B12).

VITAMIN B12 DEFICIENCY
Vitamin B-12 deficiency can be difficult to detect, especially since the symptoms of a vitamin B-12 deficiency can be similar to many common symptoms, such as feeling tired or unfocused, experienced by people for a variety of reasons.
Vitamin B-12 deficiency is commonly associated with chronic stomach inflammation, which may contribute to an autoimmune vitamin B-12 malabsorption syndrome called pernicious anemia and to a food-bound vitamin B-12 malabsorption syndrome. Poor absorption of vitamin B may be related to coeliac disease. Impairment of vitamin B-12 absorption can cause megaloblastic anemia and neurologic disorders in deficient subjects. In some cases, permanent damage can be caused to the body when B-12 amounts are deficient.
It is noteworthy that normal function of the digestive system required for food-bound vitamin B-12 absorption is commonly impaired in individuals over 60 years of age, placing them at risk for vitamin B-12 deficiency.
A diagnosis of vitamin B-12 deficiency is typically based on the measurement of serum vitamin B-12 levels within the blood. However, studies show that about 50 percent of patients with diseases related to vitamin B12 deficiency have normal B-12 levels when tested. This can cause individuals to ignore taking in adequate levels of vitamin B-12 with potential serious consequences.
FUNCTIONS AND ISSUES ASSOCIATED WITH VITAMIN B-12 STATUS IN THE BODY
- Vitamin B-12 or cobalamin plays essential roles in folate metabolism and in the synthesis of the citric acid cycle intermediate, succinyl-CoA.
- Vitamin B-12 deficiency is commonly associated with chronic stomach inflammation, which may contribute to an autoimmune vitamin B-12 malabsorption syndrome called pernicious anemia and to a food-bound vitamin B-12 malabsorption syndrome. Impairment of vitamin B-12 absorption can cause megaloblastic anemia and neurologic disorders in deficient subjects.
- Normal function of the digestive system required for food-bound vitamin B-12 absorption is commonly impaired in individuals over 60 years of age, placing them at risk for vitamin B-12 deficiency.
- Vitamin B-12 and folate are important for homocysteine metabolism. Elevated homocysteine levels in blood are a risk factor for cardiovascular disease (CVD). B vitamin supplementation has been proven effective to control homocysteine levels.
- The preservation of DNA integrity is dependent on folate and vitamin B12 availability. Poor vitamin B12 status has been linked to increased risk of breast cancer in some, but not all, observational studies.
- Low maternal vitamin B-12 status has been associated with an increased risk of neural tube defects (NTD), but it is not known whether vitamin B-12 supplementation could help reduce the risk of NTD.
- Vitamin B-12 is essential for the preservation of the myelin sheath around neurons and for the synthesis of neurotransmitters. A severe vitamin B-12 deficiency may damage nerves, causing tingling or loss of sensation in the hands and feet, muscle weakness, loss of reflexes, difficulty walking, confusion, and dementia.
- While hyperhomocysteinemia may increase the risk of cognitive impairment, it is not clear whether vitamin B-12 deficiency contributes to the risk of dementia in the elderly. Although B-vitamin supplementation lowers homocysteine levels in older subjects, the long-term benefit is not yet known.
- Both depression and osteoporosis have been linked to diminished vitamin B-12 status and high homocysteine levels.
- The long-term use of certain medications, such as inhibitors of stomach acid secretion, can adversely affect vitamin B12 absorption.
- Vitamin B12 is required for proper red blood cell formation, neurological function, and DNA synthesis.
MORE DETAILS ASSOCIATED WITH VITAMIN B12 STATUS IN THE BODY
4. Pernicious anemia is an autoimmune disease that affects the gastric mucosa and results in gastric atrophy. This leads to the destruction of parietal cells, achlorhydria, and failure to produce intrinsic factor, resulting in vitamin B-12 malabsorption. If pernicious anemia is left untreated, it causes vitamin B-12 deficiency, leading to megaloblastic anemia and neurological disorders, even in the presence of adequate dietary intake of vitamin B-12.
5. Vitamin B-12 status is typically assessed via serum or plasma vitamin B-12 levels. Values below approximately 170–250 pg/mL (120–180 picomol/L) for adults indicate a vitamin B-12 deficiency. However, evidence suggests that serum vitamin B-12 concentrations might not accurately reflect intracellular concentrations. An elevated serum homocysteine level (values >13 micromol/L) might also suggest a vitamin B-12 deficiency. However, this indicator has poor specificity because it is influenced by other factors, such as low vitamin B6 or folate levels. Elevated methylmalonic acid levels (values >0.4 micromol/L) might be a more reliable indicator of vitamin B-12 status because they indicate a metabolic change that is highly specific to vitamin B-12 deficiency.
6. Vitamin B-12 deficiency is characterized by megaloblastic anemia, fatigue, weakness, constipation, loss of appetite, and weight loss. Neurological changes, such as numbness and tingling in the hands and feet, can also occur . Additional symptoms of vitamin B-12 deficiency include difficulty maintaining balance, depression, confusion, dementia, poor memory, and soreness of the mouth or tongue. The neurological symptoms of vitamin B-12 deficiency can occur without anemia, so early diagnosis and intervention is important to avoid irreversible damage. During infancy, signs of a vitamin B-12 deficiency include failure to thrive, movement disorders, developmental delays, and megaloblastic anemia. Many of these symptoms are general and can result from a variety of medical conditions other than vitamin B-12 deficiency.
7. Typically, vitamin B12 deficiency is treated with vitamin B-12 injections, since this method bypasses potential barriers to absorption. However, high doses of oral vitamin B-12 can also be effective. The authors of a review of randomized controlled trials comparing oral with intramuscular vitamin B-12 concluded that 2,000 mcg (I like 5,000 mcg) of oral vitamin B-12 daily, followed by a decreased daily dose of 1,000 mcg and then 1,000 mcg weekly and finally, monthly might be as effective as intramuscular administration. Overall, an individual patient’s ability to absorb vitamin B12 is the most important factor in determining whether vitamin B-12 should be administered orally or via injection. In most countries, the practice of using intramuscular vitamin B-12 to treat vitamin B-12 deficiency has remained unchanged.
8. Large amounts of folate can mask the damaging effects of vitamin B-12 deficiency by correcting the megaloblastic anemia caused by vitamin B-12 deficiency without correcting the neurological damage that also occurs. Moreover, preliminary evidence suggests that high serum folate levels might not only mask vitamin B-12 deficiency, but could also exacerbate the anemia and worsen the cognitive symptoms associated with vitamin B-12 deficiency. Permanent nerve damage can occur if vitamin B-12 deficiency is not treated. For these reasons, folate intake from fortified food and supplements should not exceed 1,000 mcg daily in healthy adults.

Groups at Risk of Vitamin B-12 Deficiency
The main causes of vitamin B-12 deficiency include vitamin B-12 malabsorption from food, pernicious anemia, postsurgical malabsorption, and dietary deficiency. However, in many cases, the cause of vitamin B-12 deficiency is unknown. The following groups are among those most likely to be vitamin B-12 deficient.
Older adults: Atrophic gastritis, a condition affecting 10%–30% of older adults, decreases secretion of hydrochloric acid in the stomach, resulting in decreased absorption of vitamin B-12. Decreased hydrochloric acid levels might also increase the growth of normal intestinal bacteria that use vitamin B-12, further reducing the amount of vitamin B-12 available to the bodY.
Individuals with atrophic gastritis are unable to absorb the vitamin B-12 that is naturally present in food. Most, however, can absorb the synthetic vitamin B-12 added to fortified foods and dietary supplements. As a result, the IOM recommends that adults older than 50 years obtain most of their vitamin B-12 from vitamin supplements or fortified foods. However, some elderly patients with atrophic gastritis require doses much higher than the RDA to avoid subclinical deficiency.
Individuals with pernicious anemia: Pernicious anemia, a condition that affects 1%–2% of older adults, is characterized by a lack of intrinsic factor. Individuals with pernicious anemia cannot properly absorb vitamin B-12 in the gastrointestinal tract. Pernicious anemia is usually treated with intramuscular vitamin B-12. However, approximately 1% of oral Vitamin B-12 can be absorbed passively in the absence of intrinsic factor, suggesting that high oral doses of vitamin B12 might also be an effective treatment.
Individuals with gastrointestinal disorders: Individuals with stomach and small intestine disorders, such as celiac disease and Crohn’s disease, may be unable to absorb enough vitamin B-12 from food to maintain healthy body stores. Subtly reduced cognitive function resulting from early vitamin B-12 deficiency might be the only initial symptom of these intestinal disorders, followed by megaloblastic anemia and dementia.
Individuals who have had gastrointestinal surgery: Surgical procedures in the gastrointestinal tract, such as weight loss surgery or surgery to remove all or part of the stomach, often result in a loss of cells that secrete hydrochloric acid and intrinsic factor. This reduces the amount of vitamin B-12, particularly food-bound vitamin B-12, that the body releases and absorbs. Surgical removal of the distal ileum also can result in the inability to absorb vitamin B-12. Individuals undergoing these surgical procedures should be monitored preoperatively and postoperatively for several nutrient deficiencies, including vitamin B12 deficiency.
Vegetarians: Strict vegetarians and vegans are at greater risk than lacto-ovo vegetarians and non-vegetarians of developing vitamin B-12 deficiency because natural food sources of vitamin B-12 are limited to animal foods. Fortified breakfast cereals and fortified nutritional yeasts are some of the only sources of vitamin B-12 from plants and can be used as dietary sources of vitamin B-12 for strict vegetarians and vegans. Fortified foods vary in formulation, so it is important to read the Nutrition Facts labels on food products to determine the types and amounts of added nutrients they contain.
Pregnant and lactating women who follow strict vegetarian diets and their infants: Vitamin B-12 crosses the placenta during pregnancy and is present in breast milk. Exclusively breastfed infants of women who consume no animal products may have very limited reserves of vitamin B-12 and can develop vitamin B-12 deficiency within months of birth. Undetected and untreated vitamin B-12 deficiency in infants can result in severe and permanent neurological damage.
The American Dietetic Association recommends supplemental vitamin B-12 for vegans and lacto-ovo vegetarians during both pregnancy and lactation to ensure that enough vitamin B-12 is transferred to the fetus and infant. Pregnant and lactating women who follow strict vegetarian or vegan diets should consult with a pediatrician regarding vitamin B-12 supplements for their infants and children.
Health Risks from Excessive Vitamin B12
The IOM did not establish a UL for vitamin B-12 because of its low potential for toxicity. In Dietary Reference Intakes: Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B-12, Pantothenic Acid, Biotin, and Choline, the IOM states that “no adverse effects have been associated with excess vitamin B-12 intake from food and supplements in healthy individuals”.
Findings from intervention trials support these conclusions. In the NORVIT and HOPE 2 trials, vitamin B-12 supplementation (in combination with folic acid and vitamin B6) did not cause any serious adverse events when administered at doses of 0.4 mg for 40 months (NORVIT trial) and 1.0 mg for 5 years (HOPE 2 trial).
Interactions with Medications
Vitamin B12 has the potential to interact with certain medications. In addition, several types of medications might adversely affect vitamin B-12 levels. A few examples are provided below. Individuals taking these and other medications on a regular basis should discuss their vitamin B-12 status with their healthcare providers.
Chloramphenicol: Chloramphenicol (Chloromycetin®) is a bacteriostatic antibiotic. Limited evidence from case reports indicates that chloramphenicol can interfere with the red blood cell response to supplemental vitamin B-12 in some patients.
Proton pump inhibitors: Proton pump inhibitors, such as omeprazole (Prilosec®) and lansoprazole (Prevacid®), are used to treat gastroesophageal reflux disease and peptic ulcer disease. These drugs can interfere with vitamin B-12 absorption from food by slowing the release of gastric acid into the stomach. However, the evidence is conflicting on whether proton pump inhibitor use affects vitamin B-12 status. As a precaution, healthcare providers should monitor vitamin B-12 status in patients taking proton pump inhibitors for prolonged periods.
H2 receptor antagonists: Histamine H2 receptor antagonists, used to treat peptic ulcer disease, include cimetidine (Tagamet®), famotidine (Pepcid®), and ranitidine (Zantac®). These medications can interfere with the absorption of vitamin B12 from food by slowing the release of hydrochloric acid into the stomach. Although H2 receptor antagonists have the potential to cause vitamin B-12 deficiency, no evidence indicates that they promote vitamin B-12 deficiency, even after long-term use. Clinically significant effects may be more likely in patients with inadequate vitamin B-12 stores, especially those using H2 receptor antagonists continuously for more than 2 years.
Metformin: Metformin, a hypoglycemic agent used to treat diabetes, might reduce the absorption of vitamin B-12, possibly through alterations in intestinal mobility, increased bacterial overgrowth, or alterations in the calcium-dependent uptake by ileal cells of the vitamin B-12-intrinsic factor complex. Small studies and case reports suggest that 10%–30% of patients who take metformin have reduced vitamin B-12 absorption. In a randomized, placebo controlled trial in patients with type 2 diabetes, metformin treatment for 4.3 years significantly decreased vitamin B-12 levels by 19% and raised the risk of vitamin B12 deficiency by 7.2% compared with placebo. Some studies suggest that supplemental calcium might help improve the vitamin B-12 malabsorption caused by metformin, but not all researchers agree.
REFERENCES
FROM: https://academic.oup.com/ajcn/article/71/2/514/4729184
Plasma vitamin B-12 concentrations relate to intake source in the Framingham Offspring Study
ABSTRACT
INTERNET REFERENCES
2) https://lpi.oregonstate.edu/mic/vitamins/vitamin-B12
3) https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/